Metagenomic investigation of microbes and viruses in patients with jaw osteonecrosis associated with bisphosphonate therapy[]
Overview/Introduction of Jaw Osteonecrosis []
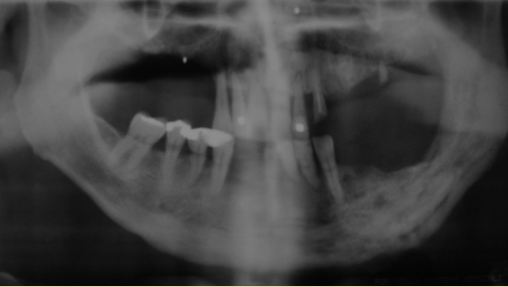
(NOTE: the images associated with this condition are pretty graphic and disturbing so they are not included, except for an xray image)
{kind=link}
Figure 1. Jaw Osteonecrosis as observed in this panoramic x-ray. Bisphosphonates and Osteonecrosis of the Jaw: A Case Report. Reiriz AB, De Zorzi Pde M, Lovat CP - Clinics (Sao Paulo) (2008) http://openi.nlm.nih.gov/detailedresult.php?img=2664202_cln63_2p0281f2&query=the&fields=all&favor=none&it=none&sub=none&sp=none&req=4&simCollection=1474711_envhper00436-0067-a&npos=53&prt=3
Jaw Osteonecrosis essentially represents what its name implies "jaw bone death". Individuals will present with exposed bone within their mouth. After the bone has been exposed for a period of 8 weeks it is classified as jaw osteonecrosis. Exposure of the bone reduces or eliminates exposure to blood and nutrients and as a result the bones become weak and die. The initial appearance of the bone will be yellow/white, but over time will become very discolored.
The disease will often appear after an invasive dental procedure such as tooth extraction, however the pathology of jaw osteonecrosis is not known. Several existing hypothesis consider the impairment of the bone to repair itself, suppression of bone turnover, soft tissue toxicity, a decrease in blood vessel formation within the mouth, infection potential, and some form of immune response.
Despite the ambiguity around disease causation, a variety of risk factors have been identified. Cancer treatment including radiation therapy and steroid use have been associated with the disease. There has also been a correlation to the disease and use of strong antiresorptive therapies (therapies that prevent bone loss). Strong antiresorptive therapies include those that use bisphosphonates or RANKL inhibitors. This translates into medications such as alendronate (Fosamax), risedronate (Actonel and Atelvia), ibandronate (Boniva), and denosumab (Prolia). Antiresorptive therapies that utilize SERMs or calcitonin are NOT associated with an increased risk. (this includes medications such as raloxifene (Evista)).
It is estimated that 1 in 1,000 to 1 in 10, 000 cases occur annually in patients taking bisphosphonates. An an increased risk is associated with individuals that have been receiving bisphosphonate therapies and are diagnosed with cancer. Given the unknown pathology and the devastating effects of the disease, a recent paper investigated microbial and viral populations in these patients. "Metagenomic investigation of microbes and viruses in patients with jaw necrosis associated with bisphosphonate therapy" uses rRNA to classify and characterize these infectious agents.
Methods[]
Subjects: 10 individuals were recruited to participate in this study at the Herman Ostrow School of Dentistry at the University of Southern California. These individuals provided researchers with saliva samples for microbial analysis and biofilm cultivation. Five of these individuals had bisphosphonate related osteonecrosis of the the jaw (BRONJ), while the other 5 served as a control, having no osteonecrosis of the jaw, despite having also received bisphosphonate therapy. Individuals from the control group were selected so that they were each similar to a patient with BRONJ in terms of age, sex, ethnicity, disease, and bisphosphonate use (type, dose, and duration). See Table 1 below. Medical records were also obtained from study subjects.
Note BRONJ was defined using American Association of Oral and Maxillofacial Surgeons diagnostic criteria. Further requirements included bisphosphonate therapy for greater or equal to one year, bone exposure as observed in stages I-III of the disease for greater than 8 weeks. Patients were rejected from the study if they had active cancer within the last 3 years, any salivary gland hypofunction, xerostomia, oral or gastrointestinal pathology, oral or systemic infection, received local or systemic antimicrobial therapies 6 months prior to the study, or had last received bisphosphonate over a year ago.

{kind=link}
Table 1. Patients Enrolled in Study, "Metagenomic investigation of microbes and viruses in patients with jaw osteonecrosis associated with bisphosphonate therapy" Dec. 2012 Lissette Valenzuelaa, An Chib, Simon Bearda, Alvaro Orella, Nicolas Guiliania, Jeff Shabanowitzb, Donald F. Huntb, Carlos A. Jerez
.
After Aquiring Saliva Samples: Samples were brought to 10% glycerol and frozen at -80*C. Saliva was thawed, homogenized and microbes and viruses were collected from different bands following density gradient centrifugation. A sample of the microbes were obtained, and then the remaining sample and viral sample were separately filtered using 3 times. Saliva samples were also used to create anaerobic biofilm starter culture and once the biofilms matured viruses were isolated as described above. (Biofilms were generated to model physiologic activity. Bacteria in the saliva will colonize oral and dental areas forming biofilms)
Viruses and Microbes were quantified using Sybr Green and epifluorescence microscopy.
Lysogeny of the viruses was explored through prophage induction. Healthy and BRONJ saliva samples were treated with mitomycin C (a DNA crosslinker and anti-tumor antibiotic reagent). Biofilms were then generated using +/- mitomycin treated saliva. Viruses were isolated from both saliva and biofilms as described above.
Microbial DNA was extracted from both saliva and biofilms in "healthy", control, and disease-presenting patients. The 16S ( a component of the 30S small subunit of prokaryotic ribosomes) V3V5 variable region was amplified and barcoded. 12 amplicons were pooled and barcoded against viral metagenomes. (DNA was also sequenced using pyrosequencing).
Results[]
Microbe and Viral Presence in Controls and BRONJ Samples

{kind=link}
Table 2. Microbes and Viruses in saliva samples.
After early microbe samples and filtered viral samples had been stained and evaluated with epifluorescence microscopy, several trends were observed. The data (as seen in Table 2) demonstrates that individuals with BRONJ have a significantly increased microbial and viral population. Prophage analysis demonstrated viral abundance decreased in mitomycin C treated BRONJ saliva samples compared with normal saliva samples. However, both biofilms, had a stronger prophage induction response than the saliva.
Classifying Microbial Distribution


{kind=link}
Figure 2. Ribomsomal Database Project Classifier evaluation of 16S sequences.
A Ribosomal Database Project Classifier assigned 31,722 chimera free 16S reads to a taxonomic group. (There were some reads that could not be resolved at the genus level with high confidence). Figure 2. Probacteria was the most represented phyla in all samples for a total of almost 99% of the overall data. This was followed by Firmicutes and Actinobacteria prescence. The microbes observed in Probacteria include the facultative anaerobes Klebsiella and Serratia. Firmicutes included Streptoccous and Bacillus.


{kind=link}
Figure 3. Ribosomal Database Classifier data in regards to saliva +/- mitomycin C treatment.
The Ribosomal Database Project Classifier information also included reads from saliva treated with mitomycin C. A range of phylla were represented in the samples. Following mitomycin C treatment, there appears to be a reduction in many microbial populations.
Brief Comments[]
This paper is very recent (December 2012 edition), however it is the first paper to characterize the bacteria in the bisphosphonate associated jaw osteonecrosis. The authors hope this information will facilitate better disease characterization, treatment, and prognosis.
Additionally, bone and soft tissue specimens from BRONJ patients primarily present with Proteobacteria, Firmicutes, and Actionobacteria, suggesting that bacteria in saliva may colonize bone.
However, when selecting for controls they did not consider the number of teeth in patients: BRONJ patients had significantly fewer teeth than their counterpart controls. This could pose a problem as microbial populations may be altered with fewer teeth.
A note was also made that DNA observed from bacteria does not necessarily correlate to viable presence in metagenomic identification.
Treatment Options[]
For many people the treatments include mouth washes, antibiotics, and painkillers.
Surgery may also be employed, to remove dead bone and create soft tissue coverage overhealthy bone.
Citations[]
American College of Rheumatology. http://www.rheumatology.org/practice/clinical/patients/diseases_and_conditions/onj.asp
Metagenomic investigation of microbes and viruses in patients with jaw osteonecrosis associated with bisphosphonate therapy. SedghizadehPP, Yooseph S, Fadrosh DW, Ziegler-Allen L, Thiagarajan M, Salek H, Farahnik F, Williamson SJ. Ostrow School of Dentistry, University of Southern California. December 2012 Oral Surgery, Oral Medicine, Oral Pathology, Oral Radiation (OOOO)
Bisphosphonate osteonecrosis of the jaw: A historical and contemporary review. Niall McLeod, Peter Brennan, Salvatore Ruggiero. February 2012. The Surgeon.